How I Healed My Subluxating Extensor Carpi Ulnaris Tendon--and Homemade Splint Instructions
Who I am
My name is Ryan Harrington and I am a Physical Therapist. I have been working in general outpatient orthopedics for 5 years. I am a very physically active person and have had my fair share of injuries. Most recently I have been dealing with extensor carpi ulnaris (ECU) instability/subluxation from the combination of CrossFit and hockey. After a lot of research and a long rehab process I can happily say that I am no longer having any pain or instability--without surgery! Due to mixed information on conservative management of this common wrist injury and my experience as a physical therapist I have decided to share my process with anyone who is struggling with this injury and is trying to avoid surgery. Please feel free to email me if you have any questions. Hope this helps!
Background
Dislocation or subluxation of the ECU tendon is one of many causes of ulnar-sided wrist pain. The ECU tendon is stabilized in the ulnar groove by a subsheath located deep to the extensor retinaculum as it passess the distal end of the ulna. The subsheath can be injured with forceful wrist supination, ulnar deviation and/or flexion. This injury is common in tennis players, golfers and weight lifters as well as in any sport that involves a lot of wrist motion. It can also occur from trauma such as a fall, bike crash or car accident. There are several treatment options available but controversy remains on how best to treat this condition. Most of my research pointed towards immobilization in wrist extension, pronation and radial deviation for 4-8 weeks(1) or surgical intervention(2). Although the case study I provided below for conservative management of ECU subluxation reported successful stabilization after 8 weeks of immobilization, several of the other case studies I found revealed continued subluxation/instability once the athlete returned to sport and surgical intervention was usually the only way to resolve continued instability. Mixed information on treatment options and inconsistent results of conservative management is what motivated me to share my experience and hopefully help someone who has a similar presentation.
The Injury
I have been an active person all my life. I started playing team sports in high school then transitioned to individual sports in college. Over the years I have got into mountain biking, snowboarding, XC skiing, disc golf, kayaking, rock climbing, weight lifting, running, and most recently, hockey. I also started doing Crossfit in the summer of 2019 and was really enjoying the high intensity and diversity of the workouts. I was in great shape and feeling stronger than ever. During this time I was also playing recreational hockey in a city league. It was this combination of activities that resulted in an acute onset of wrist pain. I developed some pain just proximal to the ulnar styloid process the day after a Crossfit workout that involved over a hundred reps of snatches and deadlifts at moderate weight. The pain was not severe but was accompanied by some visible inflammation and tenderness. I assumed I had developed an acute onset of tendinitis and decided to attend Friday night pickup hockey despite the discomfort. From my experience with these types of “injuries” I have always been able to work through them and general exercise almost always cured my ailments. I got through the hockey game without pain but started to notice some issues the next day. I was hanging drywall in my workshop with my brother when I started to notice a very disconcerting “popping” and “catching” sensation in my wrist when I got my wrist into certain positions. I started to pay attention to this sensation and realized that it happened every time I supinated (palm up), extended and went into ulnar deviation (towards the pinky side of the hand). The sensation was very unpleasant and often resulted in my wrist locking into this position until I forced it back into a more neutral position. I continued to work the rest of that day but when I finally sat down to eat dinner and relax for the evening I realized that the ulnar side of my wrist at the ulnar styloid process was very swollen and tender to palpation. I tested the provoking positions and was able to recreate the “snapping” sensation with the same combination of movements I described above (supination, extension, and ulnar deviation). Based on the sensation and presentation I thought to myself “it feels like my extensor carpi ulnaris (ECU) tendon is subluxing or dislocating from its tunnel at the styloid process”. This is how a normal person's brain thinks, right? I had never learned about this pathology in school but was pretty confident in what I was feeling. I did some quick research online and learned that ECU instability is a relatively common wrist injury and often occurs in high level tennis players. I also learned that immobilization is the primary treatment method. Oh yay, some more time in a brace/splint (I had spent 10 months in a wrist brace while I healed from a bone graft surgery to encourage bony bridging of my scaphoid that had died due to avascular necrosis. This occured 8 years ago and was on the opposite wrist). I woke up the next morning hoping that it was all a dream but when I ulnar deviated the tendon popped right out of its groove and my wrist “locked”. My heart dropped with the thought of dealing with yet another immobilizing injury.
Note: I am a licensed physical therapist trained to evaluate, diagnose, and treat orthopedic and musculoskeletal injuries. If you do not have a formal diagnosis from a healthcare provider for your pain or injury make sure you see an orthopedic physician or PT to help you get an accurate diagnosis. There are a lot of things that could cause ulnar sided wrist pain and you don't want to treat the wrong pathology. If you have questions please send me an email and I can help guide you in the right direction.
The Immobilization Process
After doing some research on managing ECU subluxation and subsheath tears I learned that the most common conservative management is immobilization in wrist extension and radial deviation. The goal of this position is to limit stress on the ECU subsheath and promote healing of the damaged structures. Being the resourceful person I am, I opted for the most practical immobilization tool I could think of-- a spatula, obviously. This common household item allowed me to get my wrist in an extended position while I looked for a more permanent and professional looking solution. You could imagine the looks of skepticism I got when I showed up to work the next day with a spatula strapped to my wrist with an Ace Bandage. But the pain relief and wrist support I got was well worth the judgement and eye rolls from co-workers and patients. After a few days of spatula-assisted immobilization and some talks with colleagues and my wife I was somewhat convinced that perhaps my injury was not as morbid as I had initially thought. I removed the brace and tested the stability of my wrist. Unfortunately, the instability remained. The sensation of an unstable wrist was new to me. It is hard to describe the sensation accurately but I could feel the instability all the way up into my ear and it was very disconcerting. Any time I activated the ECU muscle (i.e. trying to extend and ulnar deviate) I had a strong apprehensive feeling in my wrist that extended into my ear and head. This sensation was accompanied by pain just proximal to my ulnar styloid process along the tendon of the ECU just before it entered the sheath. This was also the location of swelling that made my ulnar styloid process look bulbous, rounded and not clearly defined compared to the contralateral side. This appearance remained for several months but has since returned to normal. The appearance of the ulnar styloid process was one of the ways I determined how close I was to a fully healed subsheath. Unfortunately, it took several months before the area started to look and feel like the other side. At seven months out now I can say that there is no apparent difference between the bony appearance of my wrist.
After a few days in the high-tech spatula-brace with no change in stability I decided it was time to find a more permanent solution. I knew that I needed something that I could mold into a custom position that was not too cumbersome. I knew that I needed a splint that prevented me from moving my wrist into ulnar deviation and kept me in a slight degree of extension and radial deviation. There are no manufactured braces or splints that do this so I knew that I would have to make my own. I purchased a Rolyan Splinting Sheet on Amazon that I could heat and mold to the desired position. I used a ⅛” thick, 1% perforated, 6”x9” sheet to mold the perfect splint for my needs. The 1% perforation allows the splint to be strong enough to provide real support while remaining lightweight and mildly breathable.
How to make an “ulnar block” splint for ECU instability
Let me start out by saying that the best thing about this brace is that it allowed me to continue to use my injured hand for work and normal daily activities. I could still cut food, hold a plate, do yard work, and other things requiring both hands. This made the immobilization process much more bearable and practical. I could strap the ACE bandage down tighter depending on the activity I was doing then remove it to let the wrist breathe.
The Steps
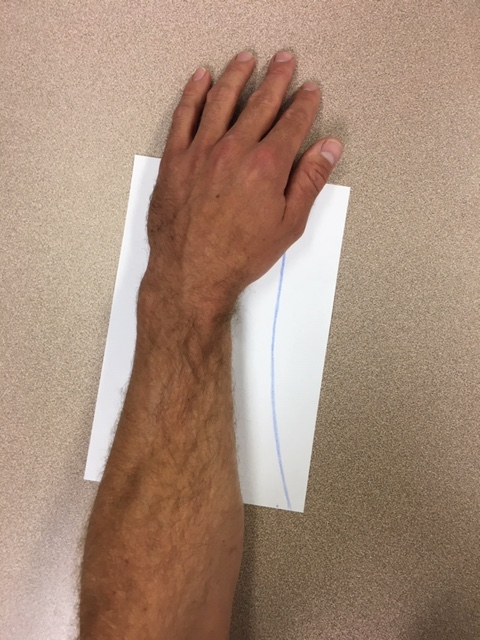
First, I marked the Rolyan sheet with a sharpie to cut down to size. To do this I placed my hand palm down on the left side of the sheet. I put my wrist in slight radial deviation and left about 1 inch of overhang on the left side of the hand/wrist that would be folded upward to work as the “ulnar block”. I placed the top of the sheet right at the MCP of the pinky (this is the first joint that transitions the palm to the pinky finger). I then used a sharpie to mark a line about 1-2 inches away from the R side of the forearm and wrist. I continued this line straight up through the thumb rather than curving around the thumb since I do not need any support on the thumb side of the wrist. Allow for excess material since you will end up trimming this down once the splint is formed. Better to have too much material initially rather than cut it too small. Cut off the excess material on the right side of the sheet.
Next, it is time to dunk the splint material in a pot of hot water to mold to the wrist in the desired position. This is the most important step because if you get the material too hot you will distort it too much while molding the material to your wrist and it will look like a Picasso painting. It will also get too thin in places and weaken the material. Better to do less time in the water initially because you can always take more dunks back in the water until you get the desired shape.
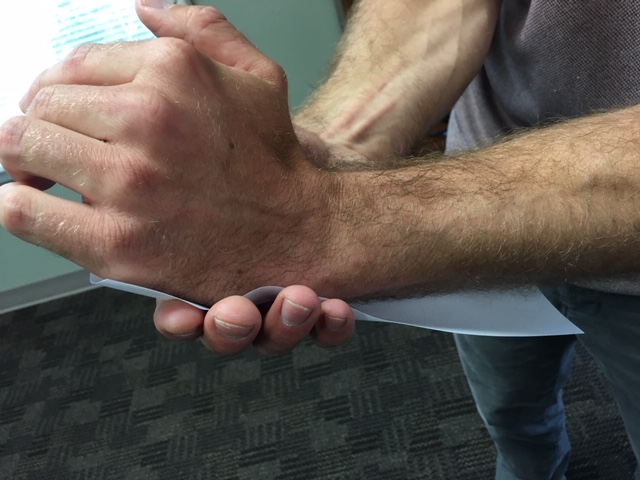
Here is how to do it: Boil a large pot of water that will allow the entire cut out material to be submerged (without touching the bottom of the pot, ideally). Once the water is boiling, turn off the burner and allow the boiling to stop and the water cool slightly (about 3 mins--I suggest setting a timer). Hold the material in the bottom right corner and dunk in the water completely, minus the small corner you are holding. You should only let it stil in the water for about 3-5 seconds initially since it does not take long for the material to become soft and malleable. Remove from water and dangle for a second to allow hot water to drip off and avoid burning your skin. Place the splint on your wrist, making sure your wrist is in about 30 degrees of extension and about 15-20 deg of radial deviation. Use your uninjured hand to wrap the material around the palm using your fingers to wrap snugly around the pinky side of the hand. The material should extend upwards slightly past the backside of your hand. Next, move to the wrist using your uninjured hand to conform the splint around the wrist and forearm. You may need to dunk the brace in the water a few times since the material hardens as it cools. Try to only dunk the area that needs to be molded so you don't lose the mold of the area you have already completed. I dunked the brace several times to achieve the desired fit and this did not compromise the integrity of the material at all. Error on the side of less time in the hot water to avoid distorting the material too much.

Now that you have a decent fit on the wrist/hand you can take some scissors and trim the brace to the desired shape. Round out the corners, shorten the forearm section for comfort, etc. The brace only needs to extend up the forearm about 5-6 inches from the crease of your wrist.
The next step is optional but I feel that it made the brace much more comfortable and sturdy. Cut a small V-slit in the corner of the top of the brace where it curves around to the pinky to allow for the top edge to fold down without stretching the material and distorting the corner. Then I dipped the tip of the brace (about ¼ to ½ inch) into the hot water and folded the top edge of the brace down and mashed it into the underside of the brace. This allowed for a more structurally sound top edge, better rigidity of the ulnar block and a more ergonomic and comfortable top edge for my fingers to curl over.






I realize that this is not the most aesthetically pleasing brace but, come on, I had no instructions and I wore it for 4 months straight! Give me a break! And it was surprisingly comfortable.
You may now be wondering how the heck to attach this ugly contraption to your wrist?! Easy, an Ace Bandage. This allows for easy donning and doffing (fancy terms for putting the brace on and taking it off) to shower and let the wrist breathe after exercise or a sweaty day. I did try velcro attachments that wrapped around my wrist but this did not feel secure enough and I ended up removing the velcro attachments after a week or two.
This material is exceptionally sticky when in direct contact with the skin so I used a sock to slip over the brace that I could change out when it started to get gross. You could use other bandaging material like gauze but to me the sock was much more convenient and comfortable. You could even accessorize the sock to match your outfit if you want!
I wore this brace 24/7 except to shower or take it off in the evening while watching a movie or show and I could prop it up with pillows to maintain the proper position of my wrist. After 3 months I started to do some passive ROM (stretching) but I will address this in another section of this blog). I found it to be very important that I wore it at night since there was much more likelihood that I would involuntarily move my wrist into a provocative or unstable position which could compromise my healing.
Rehab Timeline
Ok, it’s time to talk timeline. Unfortunately, there is a lot of mixed information as well as a lack of information out there in the research regarding conservative management of ECU instability and subsheath injury. Some say 4-8 weeks of immobilization, others say 4 months. Some say surgery is the only way to make the subsheath stable again. I was eager to get back to my normal recreational activities so I wanted to shoot for the six week timeline. During those 6 weeks I had very minimal pain but still had some obvious inflammation and my ulnar styloid process was not clearly defined. The main discomfort I had was simply from being immobilized and the resultant soft tissue tightness and joint stiffness. Every once in a while I would reflexively try to move my wrist into ulnar deviation which would result in some sharp pains at the ulnar side of the wrist just proximal to the styloid process but would go away quickly. This was also a different sensation than the instability sensation and apprehension that I would have prior to wearing the splint. After six weeks I removed the brace and started to try and do some rehabilitative therapy. However, it was very obvious to me right away that the subsheath was still compromised and it was not ready to begin the rehabilitation phase since any healing that had occured would be compromised by putting stress on the healing structure. I talked with a colleague who had completed a sports residency and he advised me that there was a lot of new research that suggested four months of immobilization was more ideal for any ligamentous tear (compared to the popular 6-8 week philosophy). Since there were no specific recommendations for subsheath injury I went with this philosophy and strapped the splint back on and committed to the four month time frame.
Treatment during Immobilization
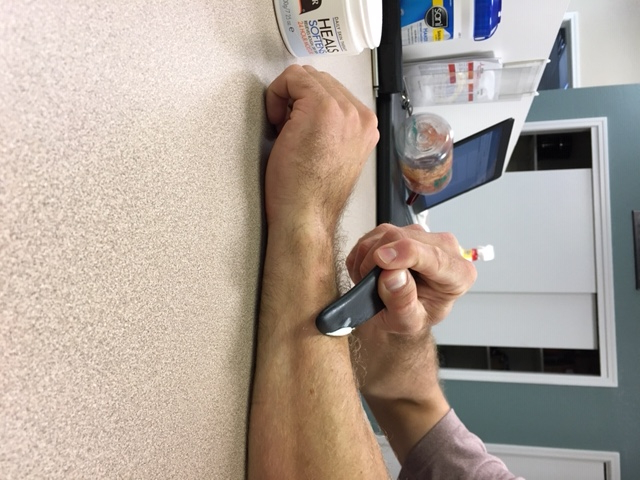
During the immobilization phase my goal was to promote tissue healing and scarring of the ECU subsheath to improve stability of the ECU tendon as it moves through the ulnar groove. The ECU subsheath is a component of the extensor retinaculum that maintains the ECU tendon in the ulnar groove. This subsheath can tear with trauma and/or repetitive use injuries. Injuries to the subsheath are common in sports with forceful pronation and supination such as golf, tennis, or hockey. Once this subsheath is torn, whether complete or partial, the goal is to reduce stress on this sheath to allow for healing to occur. If the injured person were to continue to use the wrist normally then the subsheath will continue to be traumatized which will prevent healing from occurring. Furthermore, if the individual does not immobilize for long enough then the subsheath is vulnerable to reinjury and recurrent instability when stress is placed on the subsheath again. My goal with immobilization was to allow for complete healing and scarring of the subsheath prior to placing the subsheath under any mechanical forces (i.e. ulnar deviation, supination, extension). To aid in the healing process while immobilized I performed several interventions. I utilized ice cupping, ice packs, dry needling, instrument assisted soft tissue mobilization (IASTM), massage, ultrasound and some general upper extremity strengthening that did not put stress on the ECU subsheath.
Ice cupping: Ice (cryotherapy) is a great way to help manage swelling and pain. Ice cupping is a convenient way to reduce swelling that can be done quickly while only applying ice to the target area. To ice cup simply full a small dixie cup full of water, freeze it, the rip off the top inch of the cup. Now you can massage the inflamed area with the ice without freezing your fingers off. First it will feel cold, then more of a burning or pain sensation, then it will go numb. When the area you are icing goes numb you are done. Do not keep icing since this can result in tissue damage or frost bite. Keep the ice cup moving throughout the treatment and cover an area that is slightly greater than 2x the size of the ice surface. Just toss the ice cup back in the freezer to use again.
Ice pack: pretty self explanatory. Ice for about 20 mins at a time with a nice ice pack that will conform to the inflamed area. Stop if the area goes completely numb. Ice as often as you want.
Dry Needling: Since I am a licensed physical therapist trained in Trigger Point Dry Needling (TPDN) I was able to utilize this intervention to aid in the healing process. TPDN uses solid monofilament needles (the same style of needles an Acupuncturist uses) inserted through the skin into deep muscle and fascia to release painful myofascial trigger points or tight bands of soft tissue. Since the healing of this injury involves a period of immobilization there will obviously be some tightening of muscles of the forearm and wrist. This limited mobility can result in trigger points (tight bands of tissue that develop within a muscle belly). Trigger points can be painful but they can also increase tension/stress placed on muscle attachments and other supporting structures, such as ECU subsheath, which can increase tissue irritability (inflammation) and slow or limit the healing process. To aid in the healing of my ECU injury I performed TPDN to extensor muscles of the forearm, muscles around the shoulder joint, scapular region, as well as my cervical paraspinals muscles to reduce compression on the nerve root (I obviously had someone else perform the needling in the shoulder and neck area). However, what I feel helped the most was needling the subsheath and periosteum. This resulted in a micro-inflammatory response which helps the body lay down collagen and scar tissue in the injured area. The general idea works similar to a microfracture-- an articular cartilage repair surgical technique that works by creating tiny fractures in the underlying bone. This causes new cartilage to develop from a so-called super-clot. Obviously dry needling is not a surgical technique but the physiological principles indicate that this may be beneficial for tissue healing. I had really good results and I had no adverse effects. I believe that this treatment was an integral part of my healing process and improving the strength and stability of the subsheath and extensor retinaculum. There is a lot of good research out there on the benefit of TPDN for tissue healing, pain reduction, etc but that is not the point of this post. My goal is to provide anyone with a similar injury a guide to my rehab process that allowed me to heal a potentially chronic issue without surgery. If you have specific questions on research and evidence feel free to email me and I can provide you with some articles to read.
**Dry needling, as with any invasive procedure, has associated risks. This technique should be done by a trained healthcare provider. Feel free to contact me if you have any questions regarding this treatment or how to find a provider who is trained in dry needling. And if you live in the Boise area and want to come in for some Dry Needling then don't hesitate to send me an email! There are a lot of benefits and it has been a very effective treatment for many orthopedic issues**
Instrument Assisted Soft Tissue Mobilization (IASTM): Contrary to TPDN this is a treatment that requires no training or special equipment to perform on yourself. The physiological principles are similar to that of TPDN but without penetrating the skin. There are tons of special tools available for purchase that range from 10$ to 500$. Techniques include Graston, ASTYM, and I am sure several others. You can purchase specific tools from these companies or you can do what I did and purchase Gua Sha massage tools on Amazon for 15-30$. In college for a separate injury I even used the smooth edge of a soup ladle which worked just fine. Made for an interesting conversation when my roommates returned from class to find me sitting on the couch with a jar of vaseline, a soup ladle, and a heavily lubed up arm. IASTM helps to improve blood flow, improve soft tissue mobility, reduce pain, and promote tissue healing by causing a micro inflammatory response to allow for the removal of necrotic tissue and laying down of new collagen for connective tissue healing. I performed this treatment on the muscles of my forearm, along the ECU muscle and tendon, across the subsheath and anywhere else I was feeling tightness. I feel that this treatment was very helpful and would highly recommend it. Please reach out if you have questions.
The General Treatment guidelines for IASTM:
Hold the tool at about a 45-60 deg angle from the surface of the skin. Push towards the obtuse angle with light pressure (shout out to 8th grade geometry class!). Strokes should be 1-4 inches long depending on the treatment area.
Repeat strokes until the treatment area becomes slightly red and splotchy, known as erythema. Should only take a minute or two per region. Make sure to not press too hard as to result in excessive redness or pain.
Follow up with some gentle massage with some lotion
Can ice following if you want. Not necessary and may inhibit the localized inflammatory response we are trying to achieve.
Perform this treatment 3-4 days per week as to not place extra stress on the tissue.
Continue to perform IASTM once you are out of the brace and returning to normal exercise or sport. I have been out of the brace and exercising pretty normally for a couple months now but I still perform this treatment a couple times a week.
I didn't start performing IASTM directly over the subsheath until about 6 weeks into the healing process. Mainly because the swelling was very visible and I didnt want to irritate the tissue more than it already was. Also, it hurt to do it!
Massage: Massage the arm. Better yet, convince someone else to massage it for you. That is all I will say about this. Pretty straight forward. Massage feels good, feel good means less pain, less pain means better healing and better sleep. Done. (I will also say that my pain was never really that significant since I diagnosed myself quickly and immobilized pretty quick as well)
Ultrasound: I included this one on the list since I did use ultrasound during the process, albeit only twice. There is some evidence in support of ultrasound therapy for aiding in tissue healing but I didn't dig any of those articles out of my old grad school textbooks. And since most people dont have access to an Ultrasound unit then this section is useless. If you are seeing a PT mention it to them and they will make the decision to use it or not. I did not use it more than twice.
General Strengthening: I am a very active person and love to exercise. Throughout the rehab process I continued to exercise but avoided activities that would place excessive stress on my wrist or force my wrist into ulnar deviation (towards the pinky, but you know that term by now I am sure). I continued to run, hike, squat, lunge, bridge, etc. I even did some upper extremity strengthening by attaching a loop around my elbow to strengthen the shoulder without having to grip a handle or dumbell. Feel free to reach out if you need some advice on exercising during or after the immobilization phase. I ran with the brace on, obviously, but removed the sock since this got really hot and nasty. The brace was easy to clean afterwards. Whether I actually cleaned it everytime or not is a secret I will never tell.
Treatment after immobilization phase (~16 weeks)
So, you have been stuck in this smelly, disgusting homemade brace for the last 4 months… now what?! Time to start the actual rehab process! Yay, exercise! The first thing I will say here is, start SLOW! If you have been good with the immobilization part of the process then your wrist will be pretty stiff and weak. Be gentle and work toward improving your strength and mobility slowly while letting pain and body awareness be your guide. Trust your instincts. If a movement feels unstable or “wrong” don’t do it. As you start strengthening your wrist again there is one thing that you MUST buy. It’s called Wrist Widget and it is an amazing wrist “brace” that will really help support your healing wrist while you introduce your wrist back into the exercise and strengthening realm. This brace really helped me feel more confident to start lifting again by giving me a sense of support and stability. I have been exercising without limitations for the last 2 months and I still use the Wrist Widget when doing upper body exercises and especially with free weights and weight bearing exercises such as pushups and burpees. I can't recommend this brace enough. In fact, if your ECU injury is not very severe and the long immobilization process is not necessary then the Wrist Widget may allow you to continue to exercise or play your sport with less pain and less risk for worsening your injury. The Wrist Widget works to stabilize the ECU tendon by using two velcro straps that wrap above and below the ulnar styloid process. This brace also helps stabilize the distal radio-ulnar joint by adding a compressive force. The brace does not hinder movement at all and is very comfortable. It is normally 30$ but is on sale for 22$ right now. This might seem expensive for such a small amount of material but I promise it is worth every penny.
My Treatment Protocol:
Below is a guideline to the immobilization and rehabilitation process I used. This is a guide and may be modified based on the severity of your injury. As I said previously, please make sure you have an accurate diagnosis from a trained healthcare provider to ensure that you are treating your injury correctly.
Early immobilization phase (0-6 weeks)
Goals
Reduce inflammation
Protect the damaged tissue and prevent movement into provocative/unstable position (Avoid ulnar deviation & supination)
Make an “Ulnar Block” brace
Therapy/Interventions
Ice/rest (ice cupping)
IASTM and massage to forearm muscles while avoiding the subsheath area
Any exercises which do no place stress on healing tissue
Run, hike, stationary bike, squats, lunges, balance, etc
Start to perform IASTM (and Dry Needling if you have a trained healthcare provider) to subsheath area around week 4 or when pain and inflammation has subsided.
Immobilization phase II (6-16 weeks)
Goals
Promote tissue healing
Protect the damaged tissue and prevent movement into provocative/unstable position (Avoid ulnar deviation & supination)
Therapy/Interventions
Continue with ice cupping, IASTM, TPDN, massage, etc.
Can start to implement upper body exercises with modifications to avoid putting wrist into ulnar deviation and exercises that involve holding a handle or dumbell. You will have to get creative here but body weight exercises are great
Arm circles, shoulder presses without weight, shrugs, forearm planks, core work,
Late immobilization phase (16-present)
Goals
Begin general strengthening and stabilization exercises of the upper extremity with wrist in a neutral position
Continue to wear the brace at night
Continue to avoid excessive movement into ulnar deviation
Improve overall wrist mobility into flexion, extension, pronation and supination while being cautious with progressing ulnar deviation
Continue to promote healing and scarring of subsheath
GET A WRIST WIDGET!
Therapy
Continue with ice cupping, IASTM, TPDN, massage, etc.
Use the Wrist Widget when performing upper body exercises to protect and stabilize the ECU tendon
I have continued to wear the brace at night. I feel that it helps continue the healing process after stressing the tendon and subsheat with daily activities and exercise. It also helps to create some joint stiffness and limitations into
Passive stretches into wrist flexion, extension, pronation, supination without applying excessive force which may cause pain or inflammation
Start slow- this is a marathon not a sprint. You have been immobilized for a long time and muscles need time to adapt to these stretches.
Long duration, low force stretching. Apply gentle overpressure that allows you to feel a light stretch but that you can maintain for 30-45 seconds. If you can't hold the stretch for that long because it’s too uncomfortable then you are pushing too hard. 2-4x/day should suffice.
General upper extremity strengthening that allows you to maintain your wrist in a neutral position
Rows, lat pulldown, bicep curls, shoulder press with dumbbells, table push-ups, etc (if you need exercise ideas feel free to send me an email)
Tricep presses should be done with really light weight to start (try a TheraBand or super light dumbbell since this motion applies more stress to the ulnar side of the wrist).
I did not do any wrist specific exercises such as wrist curls or wrist roll-ups. One, they did not feel good and caused some discomfort. Two, I felt that general upper body strengthening improved my sense of wrist stability without placing unnecessary, isolated stress to the ECU tendon and subsheath. They also did not feel like a functional exercise to me.
Introduce weight bearing (push up position, bike riding, etc) slowly. This is a very important position for your wrist to improve wrist stability, however, your wrist has been immobilized a long time and the carpal bones in the wrist have shifted positions slightly. Be nice to them and start slow by doing an elevated pushup (to a table or back of a chair) or dumbbell or machine chest press with light weight. Lots of options here. Email if you have questions or talk with your local trainer or PT.
Cardio is good. Bike, run, row machine, etc
Progress slowly and let pain and inflammation be your guide
Use the Wrist Widget when doing upper body exercises to help support your wrist and stabilize the ECU tendon.
References
Rolyan Splinting Material:
https://www.amazon.com/gp/product/B0793FPLFY/ref=ppx_yo_dt_b_asin_title_o04_s00?ie=UTF8&psc=1
Wrist Widget:
https://www.amazon.com/gp/product/B0056PQV2K/ref=ppx_yo_dt_b_asin_title_o05_s00?ie=UTF8&psc=1
https://www.wristwidget.com/blogs/blog-archive/could-this-be-an-ecu-injury-instead-of-a-tfcc-tear
Other articles that may be useful
https://www.jhandsurg.org/article/S0363-5023(14)00469-9/pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3418964/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3582875/
I'm having the same problem. I started noticing it 2 days after a cortisone injection in my ecu for a little tendonitis. I don't think my injury is as bad as yours. Nothing was torn in the MRI. I'm a busy massage therapist and cannot work. How long from start to finish was you process?
ReplyDeleteAlso, did your brace keep your arm from supination?
DeleteFrom start to finish my process was about 4 and a half months due to severity of my injury. It doesn't sound like yours is as significant of a tear but may still require a period of immobilization. I mainly wrote the blogpost since most of the information regarding timeframe was simply not successful with shorter immobilization periods. The brace did help prevent supination but it didn't restrict it completely Mainly it just made supination a little more awkward and was more a cue to avoid that position. If I strapped the ACE bandage down a little tighter then it certainly restricted supination more. Just make sure to have your forearm in full pronation if you make the splint. Let me know if you have more questions.
DeleteAlso, keep in mind that MRI's are not very good at ruling out ECU subluxation and subsheath tears. An MRI may be able to show a full thickness tear of the subsheath but without a forceful traumatic incident (I am guessing yours is more of an overuse injury as a massage therapist) then you likely have more of a partial tear or simply a result of increased inflammation and swelling. I would suggest that you focus on swelling management and prevent any movement that would cause your ECU tendon to subluxate for at least 2-3 weeks and then reassess the stability. If that requires you to immobilize with a brace then I suggest doing it. It is very surprising how frequently you go into that provocative position (supination and ulnar deviation) during normal daily activities. Every time you subluxate or it "pops/catches" you are causing more trauma and increasing swelling.
DeleteNo tears or tendonitis on dynamic ultrasound. Just general laxity. I recieved a prp injection with instructions to wear the wrist widget for a few week. Hope it helps! Thank you and I'll keep you posted
DeleteI ordered the brace. My need your help!
DeleteGlad you dont have major tears. Thats a good indication that it can heal on its own with the right treatment. Happy to help you out when you get the brace. Just let me know what I can do. Happy to chat over the phone if needed as well. Just email me and we can discuss. ryanharrington14@gmail.com
DeleteGot rid of herpes 1&2 completely, I started the treatment August 2022 for 14 days till now 2025 I have not had a single outbreak, All thanks to Dr. chalopa. Here is his details (drchalopa@gmail. com) WhatsApp +2348139677355
DeleteHave you tried sleeping with the splint. What was the effect?
ReplyDeleteAlso do you have an email so I could send pictures of the splint that I made copying your instructions?
DeleteYes, I slept in the splint every night. I did not have any issues with it at all and it was pretty comfortable. I even continued to sleep in it for a month or two after I started to resume normal activities to help with the healing. My email is ryanharrington14@gmail.com. Would be happy to take a look.
DeleteOkay thanks I'll send it now
DeleteActually I'll send it tomorrow
DeleteHello. My name is Katya. I'm 18 and I've been in a lot of pain near the end of April. (I'm an artist, right handed) and when I went to the clinic they told me I had carpal tunnel. It went away after rest I believe but now I think I developed the same injury in both hands. I've been to three clinics now and no one has been able to identify what's wrong with me– they just shrugged it off and told me the swelling in both wrists was "normal" and after getting covid (presumably from going to those clinics) I stopped altogether but I'm still in pain. My wrists
ReplyDeletefeel unstable as you said, but do you have a picture of what the swelling looked like? Was it exactly on the "wrist bone?" I thought I had a TFCC tear but the wrist widget only squeezes the swollen area and it hurts, and they say tfcc tears/injuries don't swell. But I'm thinking about doing what you did and making my own brace. At least when I tape it my hands seem to feel better
Hey Katya! Sounds frustrating to not get any real answers. It is hard to determine what is causing your pain from what you are describing. You can test for ECU instability but performing a simple test. Start with your elbows by your side and turn your palms up like you are holding a tray of food. Then move your wrist towards the pinky side of your hand. A positive test would be if your tendon pops out of position and then pops back into position when you return your wrists to normal resting position. With this test pain does not really give any information. It may hurt it may not. But it would certainly feel unstable and may give you an "uneasy" feeling.
DeleteAs for the swelling-- my swelling was located above and below my ulnar styloid process making that bump look much less pronounced. I can send you a picture to show you where my swelling was but I don't have a picture of when it was actually swollen. Place your hand on a table palm down. If you follow down the pinky and cross over your wrist you will come across a bony prominence known as the ulnar styloid process. If you really poke around that bony prominence you may even be able to detect that little channel that the tendon passes through between these two little mounds. Compare the left and right wrists to determine if there is a notable difference. This is where my swelling was and where the pain would be if you had the same injury as I did. Let me know what you find! And if you want a picture or have more questions you can email me at ryanharrington14@gmail.com
Forgot to mention– I sent you an email! Thanks for the response.
DeleteHi!! I am non native english speaker who have the same injury you had. I read your post but It’s hard for me to follow your brace making tutorial because I am not good at english. Could you make a video about your instruction? It will be very helpful not only for me but also for the other people. Thanks.
ReplyDeleteHey! That's a very good idea and I will try and make a youtube video with detailed instructions as soon as I find some time. I have been really busy at work and with my 3 month old baby so spare time is hard to come by. Thank you for the idea though. I will post the video here when I get it done.
DeleteThis comment has been removed by a blog administrator.
ReplyDeleteThank you for the valuable content. I also have a website from my country. If you have free time, visit บอลวันนี้
ReplyDeleteHi Ryan, thank you for your blog and writing down your experience with this. It is always good to know that one is not alone in this misery. I developed pain in my right and left wrist last July. I am sure it had something to do with more computer work and less exercise during the lockdown in WA. I finally saw a doctor in September 2020 and got a splint for my right hand (I wish I would have known your blog earlier, would have saved me $250).
ReplyDeleteI had a couple of store bought 'wrist bands' which did not really help. I was lazy with the splint in the beginning for being so uncomfortable but have been immobilizing now for about a month and I feel the pain is less and I can do most things pain free. My question is in regards the 'Wrist-Widget'. The company does not recommend it for 'ECU only' treatment and focuses on 'TFCC' but it seems your experience might be different. Would love to hear your thoughts. Thank you, I appreciate your time and congratulations on being a new Dad.
Thanks for reaching out and sorry for the delayed reply. I recently moved to Colorado.
DeleteI used the wrist widget once I was done with the long immobilization period to help provide some support and stability while I returned to normal exercise regimen. I used it for probably two months when I did any weight bearing exercises (pushups) or dumbell work. I no longer use the wrist widget now that I am back to my normal lifting routine without issues.
I would not recommend the wrist widget to attempt to heal and ECU subsheath injury and would only use it once the subsheath is healed to get back to daily activities and exercise. Hope this helps.
I replied via email but will include my response here for others to view:
ReplyDeleteHey David,
Sounds like a pretty annoying injury. I know the feeling. I am glad you have an MRI that confirms extensor Capri ulnaris tendon subluxation and possible subsheath injury cause an accurate diagnosis is the most important factor in determining treatment direction. From my research, surgery is very hit or miss on its success rates and from what I hear the healing/rehab process kind of sucks. I did not want to go the surgery route either.
I will start out by telling you that my ECU/subsheath/wrist feels great and I am not limited in my activities at all. I do avoid certain heavy lifts and ballistic movements (such as kipping pull ups, repetitive/heavy barbell work, etc) but that is fine by me. I no longer do CrossFit since I do believe this was likely the cause of my injury. I am still working out consistently and able to do all my normal lifts with a lot of dumbell work. As far as daily things I am not limited at all. I redid my entire backyard which required hours and hours of shoveling and that posed no issues to my wrist at all. It does occasionally “pop” but this pop is nothing like the original sensation of the tendon subluxing and is not painful or uncomfortable at all. And only occurs infrequently. I am also going on 36 so there are a lot of things that are popping and clicking in my body haha. The only activity I have not tried to get back into is hockey due to COVID. But I do think that my wrist would hold up fine.
My treatment rationale goes as follows:
If the subsheath is torn, then it will need adequate time to heal in order to be structurally sound again. There is strong research that shows that ligaments (connect bone to bone such as the ACL, MCL of the knee) and connective tissues similar to the subsheath require longer healing times than a tendon/muscle injury due to lesser blood supply and different tissue composition. This extended healing time can be as short as 10 weeks and as long as 16-20 weeks. This is the rationale I used in determining to brace/immobilize my wrist for 12-16 weeks to determine if this would heal the subsheath and maintain the tendon in its proper groove.
In order for the subsheath to heal correctly you would need to ensure that the tendon is resting in its groove during the healing process. This requires a brace that maintains your wrist in slight extension, radial deviation, and pronation (your OT wife can help you with these terms). My blog will walk you through the steps in making this type of brace. Here is a link to the brace material I used.
https://www.amazon.com/Rolyan-Splinting-Material-Polyform-Perforated/dp/B0793JXZ6S/ref=sr_1_3?dchild=1&keywords=rolyan+1%2F8&qid=1615913582&sr=8-3
The most important factor in the process is that if you decide to immobilize for a long duration like 3-4 months then you would need to commit fully to this. You can’t take the brace off to test the stability of the ligament or to use your hand/wrist for some activity. Every time the tendon subluxes out of the groove it is tearing whatever connective tissue healing that has begun and you are essentially starting over. So if you decide to go this route you have to commit. You will wear the brace during the day and at night. When you take the brace off to shower or just chill around your house then you need to make sure that your wrist remains in that same position the brace holds you in to prevent if from causing any stress to the healing tissue.
Take a look back through the blog to see my specific instructions on creating the splint. If you need more help let me know. I could possibly even facetime if needed.
Let me know if you have more questions. Thanks for reaching out.
Ryan
i only have pain when I palpitate or touch the corner of the ulnar palm - is that an indication that there is a tear or should i do an MRI?
ReplyDeleteNo that is not an indication of a tear. That could be a number of things but doesn’t sound like a subsheath tear without the instability
ReplyDeleteRyan, thank you for your detailed account of your injury. I'm currently dealing with ulnar-sided wrist pain and trying to figure out what it could be. I'm a high-level tennis player, and first started experiencing ECU pain on my left hand as a result of my two-handed backhand. No particularly traumatic event, just developed over time due to over-use. I noticed the pain about four weeks ago, and I've been immobilizing it with an over the counter brace for three weeks in flexion and slight radial deviation, avoiding any supination.
ReplyDeleteWhen initially trying to figure out the source of my pain, I attempted to replicate any popping or clicking sensation as you described by ulnar deviating, flexing, and supinating my wrist. Immediately after the injury, I did not experience any popping and clicking (beyond the cracking that both of my wrists have done for years due to tennis). However, I have occasionally felt a popping near where the ECU subsheath is located, although I haven't been able to consistently replicate it, and it never felt painful, just a little strange. I have never felt this specific popping on my right wrist.
I got my wrist checked out by a doctor who diagnosed it as tendonitis and told me my pain would decrease after about three weeks. The diagnostic method was to apply a resisted force to the wrist in various directions and monitor pain, so no imaging has been done. During this test, the only time I felt significant pain was when resisting ulnar deviation, and very slight pain when resisting an inward force on my thumb/pinky. This week I removed my brace and began doing some light mobility/testing of the joint; again, very occasional popping (only remember it happening once) but I was unable to replicate the experience and certainly didn't have any kind of wrist locking. I'm writing because earlier today when opening the trunk of my car with my brace on, I experienced significant pain, again resisting a force that was pushing my wrist into ulnar deviation. I have never experienced any pain during actual ulnar deviation, only while resisting it.
Another relevant note: I've also never experienced the "instability" that you've described; I felt tendon pain, but never felt that my wrist was unstable in any way. It seems to mostly exist when resisting ulnar deviation, which makes sense conceptually as that is the same motion that my left wrist makes on my backhand. Based on what I've said, do you think this could be an issue with the ECU subsheath, or is it more likely something like tendinopathy? Do you have any recommendations for treatment or for further diagnosis? Let me know if you have any clarifying questions, and thank you in advance.
I really wanted to thank you for sharing your healing journey! It is the kind of help that I have been looking for, for years!
ReplyDeleteI had an MRI done last year, revealing: "negative for TFC injury, small perforation of membraneous portion of SL ligament, SL ligament asymptomatic, ECU subluxation over top of styloid. Small focal area of increased T2 marrow signal in the distal ulna a few mm in diameter suspicious for mild marrow edema in setting of bone contusion. Regional bone marrow signal intensity is otherwise within normal limits."
I think this was from a bicycle accident back in 2015 and was further exacerbated by my occupation (farming).
When I was experiencing severe pain back in 2015-2016, I was told by my PCP that I was just getting older (at the time I was 25! Haha!) At long last he ordered an x-ray (it came back normal) and I started physical therapy. The PT was causing more pain and I had a feeling that the underlying issue was not being addressed, so I discontinued therapy (in 2016).
Today, the orthopedic surgeon told me there is nothing I can do about it except wait for it to become so unbearable that I will need cortisone shots and/or surgery, neither of which I am interested in! He said bracing it would not help. Pretty bleak, haha!
Do you think immobilizing the wrist and following your plan could help an old injury?
I have been using the wrist widget for the past two weeks and it has been a game changer, but I still feel the ECU tendon popping out of place and causing pain, albeit much less and I do feel more stable.
I really appreciate any help.
Kind Regards,
Olivia O'Dwyer
Hi Olivia,
DeleteSorry I took so long to respond. Honestly, I thought I already did haha. But to answer your last question- I do feel like it could help to immobilize and follow my protocol. I would be a huge commitment but you have already been dealing with pain and instability for so long that if you could take two months to splint it and get some relief then that would be worth it. And now that it is winter maybe its a good time to splint as a farmer??! maybe not haha. I dont know anything about farming.
The main issue is how old the injury is. This would mean that you would need to utilize strategies to get the injury back into an acute inflammatory phase. Right now it is in a low-grade chronic inflammatory state but in order to promote new healing it would need to be put back into the acute inflammatory stage. You want blood flow and macrophages and neutrophils to come in and clean up the old crap and bring in new tissue. You would do this by using IASTM (instrument assisted soft tissue mobilization/massage), dry needling to the subsheath area, ultrasound, etc.
If you decided to do it you would need to go all in and avoid ulnar deviation movements 100% of the time. You would sleep in the brace and only take it off to shower but still keeping the wrist in slight extension and radial deviation to prevent any trauma to the healing subsheath.
I can tell you that I am still free of pain and am back to doing whatever I want. I still get some popping now and then it but its not painful and doesnt impact my movements.
Thanks for the question! feel free to ask any more questions you may have.
Ryan
Hi question with a smashed arm metal crushing arm got slight tear subseath ecuout of groove dr did not splint while at work vibration reinjured returned to dr 6 month later i loose grip strenth out of nowhere and ocasional burn from middle knucle to elbow will it ever heal
DeleteHi Olivia,
ReplyDeleteSorry I took so long to respond. Honestly, I thought I already did haha. But to answer your last question- I do feel like it could help to immobilize and follow my protocol. I would be a huge commitment but you have already been dealing with pain and instability for so long that if you could take two months to splint it and get some relief then that would be worth it. And now that it is winter maybe its a good time to splint as a farmer??! maybe not haha. I dont know anything about farming.
The main issue is how old the injury is. This would mean that you would need to utilize strategies to get the injury back into an acute inflammatory phase. Right now it is in a low-grade chronic inflammatory state but in order to promote new healing it would need to be put back into the acute inflammatory stage. You want blood flow and macrophages and neutrophils to come in and clean up the old crap and bring in new tissue. You would do this by using IASTM (instrument assisted soft tissue mobilization/massage), dry needling to the subsheath area, ultrasound, etc.
If you decided to do it you would need to go all in and avoid ulnar deviation movements 100% of the time. You would sleep in the brace and only take it off to shower but still keeping the wrist in slight extension and radial deviation to prevent any trauma to the healing subsheath.
I can tell you that I am still free of pain and am back to doing whatever I want. I still get some popping now and then it but its not painful and doesnt impact my movements.
Thanks for the question! feel free to ask any more questions you may have.
Ryan
I hold a cup of coffee and if my arm relaxes my grip drops everthing extending out causes pain if any tenion is applied how long to heal its been 6 months
DeleteThank you for sharing your detailed journey, it is really the kind of advice I was looking for a long time. I injured my right wrist in the beginning of 2018 during boxing training but did not take it seriously and kept weight lifting for another 8 months expecting it to heal (very immature). I did consult a PT and was advised to rest it for 3-4 month and then do some strengthening ( I did not use a brace when I was resting it). Although there was a 30% relief from symptoms through rest and strengthening exercises, it never fully recovered. I rested it for around 6 month (without brace) but there were certain activities like typing and writing that may have inhibited the healing process. I also got a cortisol injection and have rested it ever since but there has been no further progress. I have read your guide 2 months ago and am in a wrist brace for the past 2 month and doing all the treatments that you have suggested. Although I can rotate my hand in all motions pain free, I can still feel the pain when I put pressure on my hand (no further progress since PT). I have been suggested a PRP treatment to speed up my healing process which I will soon undergo. I have been very frustrated as my only passion is boxing and lifting but have gained 30 kg since injury. I would very much appreciate any further advice as you are someone that has been through the whole procedure. Here are my MRI results that I underwent around 10 months ago post cortisol injection:
ReplyDeleteECU tenosynovitis and partial thickness tears progressed since last MRI.
I injured my wrist playing tennis and going after a ball hit at my feet suddenly with a whipping motion because I was not paying attention and reacted in delayed way and then felt the pain on ulnar side. I have no pain with extension or flexion- only if I twist my hand toward ulnar side - supination. I can't get to doctor until this coming wednesday, so it will be over a week since I injured it. I came upon your blog when I realized that most likely this is injury to subsheath of tendon. i have no weakness at all. I have a little swelling but barely any, but possibly my ulnar head has some swelling? Or where the groove is? Can not see or feel tendon coming out of the groove, but, it just feels weird, sort of pop-feeling, not painful, just weird, then the area feels sore probably because it is being stretched. So, I am not supinating it :) I am supposed to be playing a lot of tennis in 2 weeks. But, now I am worried that will not be enough time to be sure that I don't undo healing that I can get happening. It is sore over the ulnar head as well - depending on my hand position (supinated not good, pronated feels normal, so, I am guessing that I am actually feeling pain from the sheath/tendon. So, based on everything I am reading, playing tennis is probably a dumb idea until this heals?
ReplyDeleteAre you still monitoring this? I would be happy to Venmo a modest hourly rate for 15 minutes of your time if you tell me you email. Thanks!
ReplyDeleteryanharrington14@gmail.com
DeleteHello Ryan,
ReplyDeleteI had a question. I’m in week 2 of the splinting process. I just wanted to know if throughout your splinting process you felt some slight subluxation even when wearing the splint. Occasionally, I will get a popping sensation, but doesn’t hurt at all. I’m wondering if that’s normal every day popping, or if I’m actually subluxating. And essentially hitting the reset button on my progress? Any help would be appreciated. Thank you!
This was not an issue I had during my bracing period. I can’t say with any confidence whether that is a subluxation or if the popping is from another cause. I would say that when my tendon was subluxing it felt very distinctly like instability and was very different than popping related to stiffness, arthritis, etc. Sorry I can’t help much more than that without seeing it and knowing more info. Thanks for the question.
DeleteThank you for the reply Ryan! I did not mention the root issue was a central tfcc tear that I kept neglecting to treat, which eventually led to ECU subluxation. I’m thinking the crunching / popping sensation that’s painless, is the tfcc tear / cartilage rubbing against each other. It’s been tricky trying to tackle both issues, but I need to start with the ecu tendon first before I can address the tfcc issue. Thank you for the article, it’s been a major help, since not much info is out there for conservative treatment of the ECU subluxation!
ReplyDeleteYes, that would make more sense to me as well. Darn man that sounds frustrating. Both are nagging injuries that are ambiguous at best to treat successfully. I wish you all the best.
DeleteThank you! Just a quick little update for anyone here who is also suffering from this injury. I did get an MRI. It appears my condition may be a little different than what I originally thought. However, treatment might be the same. In my case, I pushed through the pain in my TFCC for so long without addressing it , that it eventually affected the ECU tendon as a result. The ECU is a component of the TFCC, so that’s to be expected. Below are results of my MRI. The key difference is that I do not have a subsheath tear, rather laxity. (Looseness). This is due to chronic instability from the TFCC after neglecting this issue for so long. I will still try splinting and immobilizing in the hopes scar tissue can form and “tighten” the tendon back in place. However this injury occurred in Jan 21 2025 , and I am just addressing it April 10th. Hopefully it is not too late 😬. Long story short for anyone out there, if you have wrist pain even mild. ADDRESS it asap!! Take this from someone who is a total gym nut. Lifting for 10 years. No pain no gain is completely untrue. 😅
DeleteHopefully this helps anyone out there, who was like me looking all over the internet for answers. I will update after 4 months to report my results/progress. For context, I am a 29 year old Male, and the ECU injury occurred January 21 doing reverse lat pull downs.
IMPRESSION:
1. ECU, mild tendinosis distal to the ulnar styloid with mild surrounding synovitis. Lateral subluxation from fiber
osseous groove on dorsum of distal ulna consistent with laxity of the tendon subsheath.
2. Small focus shallow ulnar surface fissuring central disc, TFCC, adjacent to radial attachment, without
complete tear of the central disc.
@Ryan: Thank you so much for the blogpost - it has been very interesting to read.
Delete@Carlos:
Wow thanks a lot for sharing your story. May I ask what happened since then?
My story is somewhat similar, except that it seems I have genertically an ecu subluxation as both left and right the tendon is popping out with only a halfway supination. This is due to either: looseness/laxity of the sub-sheats and/or a too shallow ulnar groove where the tendon cannot sit deeply in. This, what i have been told by a handspecialist (without x-ray/mri) are my genetics.
I injured my left ecu in february 2025 and after healing and improvement (with basically just waiting it out) I fell on my left hand in August 2025 - basically reversing the whole healing process and I was back to square 1.
I am really contemplating and frustrated on what to do. I have been massaging the tendon by hand (gently) and very very light mobilization exercises for finger and wrist mobilitiy. But at this point I feel like giving up sometimes. it is so so so easy to re-injure and resetting the process and I heavily consider to see if a surgery could help.
So basically, I hope your issue got better since your last update. I would be very curious to hear about your experience to hopefully learn a bit from it too.
All best,
Jakob
@Jakob. Sorry to hear the that! Sadly I did not get any better with conservative treatment I opted for surgery back in November 11. My surgeon fixed my ecu and tfcc using sutures only. However I’ve been in cast that won’t be removed until end of January. It’s too soon to tell if this worked, but fair warning, if you opt for the surgery prepare for a temporary life of misery. If you happen to have a loved one who can care for you I strongly suggest it. You will be extremely limited. Recovery is slow. Doctor said I might not even notice the benefits until 3+ months have passed. So i guess we will see at that point if the surgery was worth getting. Too early for me to give my opinion since im only about a month in post op. Hope this helps!
DeleteHey, Oh I am sorry to hear that you couldnt recover by using the conservative treatment. I can only imagine things to be really difficult with the surgery option - thanks for the heads up and info for it. And uff, that slow recovery is also just painful - i hope for us to get better with it steadily! - I guess for myself things are going very slowly better by itself but also just so slow and easy to re-injure and reset progress.
DeleteThis really helps a lot. I think this is sometimes amazing with the internet, to be able to connect with people and share who have similar things going on which are quite specific and not normally around in my everyday life.
Merry Christmas and much health! :)
Hi! I found this blog after realizing I have some painless subluxation in my right wrist (pinky side). A few weeks back, I spent a few hours trying to remove a license plate screw first with a screwdriver and then with vice grips after stripping the screw. Needless to say, my arm was stiff the next day, but there was no acute "ow!" during any of the process. As mentioned, there is still no pain associated with the subluxation, and I can't get it to occur every time I rotate my arm. Given the information from some of the bloggers here, I am thinking I may have a "lax" sub sheathe like the commenter going by Carlos Meza. Is it possible for a lax sub sheathe to tighten back up, given its already been 4 weeks since the day I likely damaged it?
ReplyDeletehi
ReplyDelete